How to Build a HIPAA-Compliant Medical Voice Assistant for Real-Time Doctor–Patient Conversation Transcription
A HIPAA-compliant medical voice assistant is quickly becoming one of the most important innovations in modern healthcare software, and honestly it is getting kind of hard to ignore. Because, doctors were never really supposed to spend more time typing notes than talking with patients, you know?
Yet that’s exactly what is happening. Between updating EHRs, handling documentation, and managing compliance-heavy workflows healthcare professionals are kind of drowning in admin work. The result, burnout, rushed consultations, and less time for actual patient care.
This is where AI medical scribe solutions are changing everything. Instead of manually documenting every small conversation, healthcare providers are now leaning on medical AI systems. These tools listen to doctor–patient interactions in real time, transcribe conversations accurately, recognize medical terminology, and create organized clinical notes automatically.
Also, no, it is not just basic speech-to-text tech. Modern medical speech recognition software uses more advanced AI models trained specifically for healthcare environments. These systems understand clinical vocabulary, detect multiple speakers, and summarize conversations. They also sync directly with EHR platforms while maintaining strict HIPAA compliance standards.
That’s why the need for AI clinical documentation platforms, virtual medical assistants, and AI voice agents in healthcare is growing so fast. Hospitals, telehealth platforms, and healthcare startups are all feeling it.
Why Building One Is Harder Than It Looks?
But building a reliable HIPAA-compliant medical voice assistant is far more complex than just connecting a transcription API to an app. Healthcare applications deal with highly sensitive patient information. One weak security layer, inaccurate transcription, or a non-compliant workflow can cause serious legal, operational, and patient safety risks. It is not a small deal at all.
From secure infrastructure and encrypted data pipelines, to real time transcription engines and healthcare specific AI workflow assistant healthcare models, every layer of the system needs careful design. In this blog, we’ll break down how to build a scalable and secure AI medical scribe for real time doctor–patient conversation transcription. We’ll also cover the technologies powering modern medical voice recognition software, plus the key compliance, architecture, and deployment considerations healthcare organizations need to understand before building healthcare AI solutions.
What Is a HIPAA-Compliant Medical Voice Assistant?
In the United States, physicians spend on average about 4.5 hours each day doing documentation, which is almost the same time as they’re in front of patients. The figure comes from a 2024 Annals of Internal Medicine study, which looked at more than 40,000 clinicians. A HIPAA-compliant medical voice assistant does not only cut down that workload. It also removes the documentation debt. That’s the sort of thing that quietly stacks up when note taking keeps bumping heads with care itself. Still, the difficult part is that constructing one safely is much more complex than simply rolling out some general purpose AI scribe type tool. The level healthcare AI truly requires is not small.
A HIPAA-compliant medical voice assistant is really a clinical AI system that captures doctor–patient conversations as they happen. It transcribes speech with medical speech recognition software, then turns the raw talk into structured clinical notes. All of that needs to run inside a data handling setup that satisfies HIPAA’s Privacy and Security Rule requirements.
This is not really the same thing as simply adding a voice interface to a general chatbot. Every layer of the system, from audio streaming to EHR write-back, keeps dealing with Protected Health Information. That basically changes how teams design the infrastructure and how they handle access controls. It also determines which encryption standards get used and what audit requirements end up being mandatory.
The Market Is Moving Fast for a Reason
And you can see the market is feeling that urgency. The global AI medical scribe market is projected to reach $3.8 billion by 2030. That’s a CAGR of 32.4% (Grand View Research, 2024). Health systems are speeding up adoption because the documentation burden is measurable. The regulatory fallout from non-compliant AI voice agents in healthcare can be severe. Also, the average healthcare data breach now costs $9.77 million per incident. That’s the highest across all industries for the 13th year in a row (IBM Cost of a Data Breach Report, 2024).
Why PHI Risk in Voice Systems Extends Far Beyond Storage?
Most teams kinda underestimate where Protected Health Information actually ends up in a voice pipeline. Like raw audio is PHI. Temporary transcription buffers are PHI too. System logs that mention encounter IDs are PHI, and sometimes those logs sit in places people don’t even think about. Also, even model inference responses can carry PHI if they happen to include patient names or diagnostic terms.
So compliance can’t just be a “storage-only” thing. It has to cover the parts of the flow that nobody treats as the main record. For example, it must include: live audio streaming channels between the device and the processing backend, intermediate NLP buffers that keep partial transcripts while inference is running, API calls into EHR systems that pass along patient identifiers, and monitoring dashboards or error logs that can echo clinical content.
It also includes the model retraining datasets derived from real encounters. Basically, every component that touches audio or transcript data carries the same HIPAA obligations as the final stored record. Even if it feels more like “just temporary.” Teams that realize this late in the build usually end up with expensive re-architecture. That’s the part that hurts.
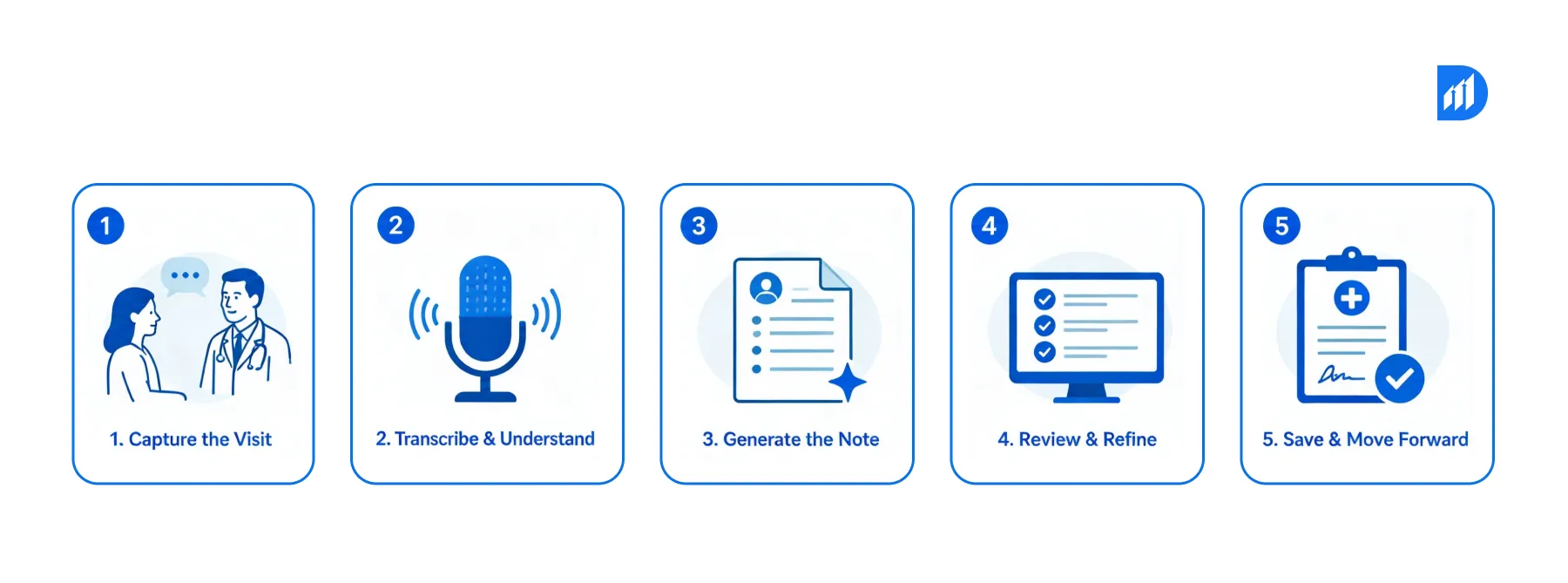
The Core Architecture of a Medical AI Scribe: 5 Functional Layers
Before implementation, you need a sort of clear picture of how these systems are structured. Like you have to understand it first, not just “run it”. AI clinical documentation pipelines for healthcare generally use a consistent, five layer architecture, at least in most production setups.
Layer 1: Audio Capture and Streaming
A device microphone captures the consultation, then audio streams over an encrypted TLS channel to a cloud hosted or on premise ingestion service. Speaker diarization separates the clinician’s speech from the patient’s. Noise suppression filters out exam room ambient sound that would otherwise mess things up.
Layer 2: Medical Speech Recognition
A domain tuned speech to text engine converts audio into text incrementally rather than in batches. Standard commercial ASR engines usually hit word error rates around 20–30% for medical terminology unless they get fine tuning. Domain adapted models, built on medical vocabulary sets, reduce that to under 5% (JMIR Medical Informatics, 2023).
Layer 3: Clinical NLP and Structured Documentation
The raw transcript kind of flows through a clinical NLP model. It pulls out named entities like diagnoses, medications, dosages, symptoms, allergies, plus treatment plans. After that it organizes everything into standard note formats such as SOAP (Subjective, Objective, Assessment, Plan) or maybe specialty-specific templates, depending on the context it senses.
Layer 4: Physician Review Interface
The structured draft shows up in a review panel, could be embedded right inside the EHR, or it appears as a standalone interface. Physicians can then edit, confirm, or reject sections before the note gets finalized. Those editing behaviors then feed back into the model retraining pipelines, which in turn improves future extraction and structuring.
Layer 5: EHR Integration and Write-Back
Once approved, the finalized notes synchronize into the electronic health record using FHIR R4 APIs or HL7 v2 messages. The system maps them to the right patient, encounter, and template. If a write fails, retry logic kicks in, with idempotent transaction controls so duplicate documentation does not accidentally show up.
When to Build a Custom HIPAA-Compliant Medical Voice Assistant?
Not every organization should build from scratch, honestly. Building a custom healthcare AI voice agent kinda makes sense when your setup is specific, like:
- Your organization needs on-premise or a private cloud deployment for data residency reasons, not just “somewhere in the cloud”
- Your specialties rely on non-standard documentation formats that off-the-shelf AI scribes just can’t handle, not even close
- You require deep EHR integration beyond what vendor solutions provide, like bi-directional medication reconciliation where it’s not only read but also updates
- Your patient population has particular linguistic patterns or accent characteristics that push you toward custom model fine-tuning
- You need audit-level control over every stage of data processing for compliance or accreditation commitments, so nothing is a black box
In short, building custom can deliver measurable returns. Health systems with mature AI clinical documentation programs often mention about a 45-minute reduction in daily charting time per physician. That’s on top of a 72% drop in after-hours documentation burden (Nuance Communications Enterprise Study, 2023).
When NOT to Build a Custom Medical Voice Assistant?
This section matters just as much as the “when to build” guidance. Most competitor blogs sort of skip it all together, anyway.
Do not build a custom AI medical scribe if:
- Your organization lacks an internal MLOps team capable of managing model drift and retraining cycles. Medical AI degrades without continuous oversight, like it just slides.
- You are deploying in fewer than five clinical departments. The infrastructure overhead honestly rarely produces ROI at that size.
- Your EHR system is being replaced within 18 months. Your team will basically need to redo all integration work from scratch.
- You need to go live in under 90 days. Production-grade HIPAA-compliant systems require security testing, BAA execution with all vendors, plus clinical validation. Rushing these steps creates regulatory exposure.
- You cannot support a human-in-the-loop review workflow. AI scribes require physician sign-off before documentation becomes part of the legal medical record. Any deployment without that control is a compliance risk.
In these situations, a validated off-the-shelf HIPAA-compliant medical voice assistant platform or a managed AI scribe service delivers faster, safer results.
Step-by-Step Implementation: Building the HIPAA-Compliant Pipeline
Building a HIPAA-compliant medical voice assistant requires much more than integrating speech-to-text technology into a healthcare application. Every layer of the system, from audio streaming to medical AI processing and EHR integration, must be designed around clinical accuracy, low latency, and strict HIPAA compliance standards.
The implementation process involves setting up secure healthcare infrastructure, deploying medical speech recognition software, and building AI clinical documentation workflows. It also means ensuring sensitive patient data stays protected throughout the entire transcription pipeline.

Step 1: Map Clinical Workflows Before Touching Infrastructure
Try to capture what physicians do in practice, not what the policy reads. Sometimes you notice these are a little different. List the consultation types, the average visit length, and the specialty-specific terminology density. Also note the point in the visit when documentation usually kicks off. That whole mapping decides where the mic should sit and what diarization requirements show up. It also tells you which NLP entities the model has to pull reliably.
For example, a cardiovascular consult creates a much different documentation demand than a pediatric well visit. One model does not really cover both cases without specialty fine-tuning.
Step 2: Stand Up HIPAA-Eligible Infrastructure
Pick cloud environments that already have executed Business Associate Agreements in place. For Azure, that usually means deploying within Azure Health Data Services, with a HIPAA-eligible setup and configuration. On AWS, you can lean on AWS HealthLake or build compliant workloads inside a dedicated VPC. Durapid has a team of 120+ certified cloud consultants plus 150+ Microsoft-certified professionals. They deploy both of those patterns fairly often, especially for enterprise healthcare clients.
At this stage, key infrastructure controls to implement include: AES-256 encryption for all recorded audio and transcripts, TLS 1.2 minimum for every service-to-service conversation, role-based access control enforced at the identity provider level, not only in the application layer, centralized key management with scheduled rotation, so it’s not managed by the application, network segmentation between the ASR service, the NLP service, and the EHR integration layer.
Step 3: Build the Real-Time Streaming Pipeline
Batch audio processing does not really work in live consultations. Physicians won’t wait 30 seconds for transcript updates, i mean that’s kinda unrealistic. Latency tolerance in clinical documentation is under 2 seconds for partial transcripts.
So you need WebSocket or WebRTC for persistent, low-latency audio streaming. Then implement rolling 500ms buffers to allow continuous inference without blocking the audio feed. Speaker diarization should run concurrently with transcription, not one after the other.
At Durapid, our AI workflow assistant healthcare implementations use Azure Cognitive Services Speech SDK with a custom endpoint deployment for medical vocabulary. That setup achieves an average end-to-end latency under 1.4 seconds, from speech to partial transcript display.
Step 4: Deploy and Fine-Tune Medical Speech Recognition
Generic speech engines really are not viable for medical voice recognition software. Drug name strings like tacrolimus, eszopiclone, or buprenorphine are regularly misheard by the system. Plus, those procedural abbreviations that are special to certain fields tend to generate systematic errors. That basically chips away at clinical trust, bit by bit.
Fine-tuning typically means you need all of this:
- Specialty-specific audio datasets with phonetically accurate annotations
- Custom pronunciation lexicons for medication names, procedure codes, and anatomical terms
- Accent-stratified training data that matches your patient and clinician population
- Ongoing word error rate benchmarking using a held-out clinical test set
When medical speech recognition software gets proper tuning, it can reach under 4% word error rate on specialty clinical vocabulary. Meanwhile, an unconfigured commercial engine on the same inputs often lands around 18–25%.
Step 5: Build the Clinical NLP Documentation Engine
So the NLP layer is where a transcription tool kinda turns into an AI medical scribe. The model can not just spot clinical terms, it has to grasp what’s going on around them. Like, if a medication gets mentioned in the history part, that’s not the same thing as a medication that is newly prescribed. Even if the drug name looks identical.
The NLP pipeline should cover things like:
- Named entity recognition for medications, diagnoses (plus ICD-10 coding support), procedures, labs, and allergies
- Negation handling (if the patient denies chest pain, that should not become a chest pain entry)
- Temporal context classification so it can tell past history from current complaint, along with whether something is planned for the future
- SOAP section routing based on conversational context, not simple keyword matching, because the same phrase can mean different sections depending on how it’s said
Durapid’s medical AI implementations on the Azure OpenAI Service use fine-tuned GPT-4 deployments, with clinician-annotated training sets tailored to the target specialty. This approach consistently beats rule-based NLP for entity extraction precision by 22–28 percentage points in post-deployment evaluations.
Step 6: Enforce Comprehensive HIPAA Security Controls
By this stage, every layer of your HIPAA-compliant medical voice assistant touches PHI. Security controls must be systematic.
Control Area | Specific Requirement | Implementation Data Encryption | All PHI encrypted at rest and in transit | AES-256 at rest, TLS 1.3 in transit Access Management | Least privilege per role, MFA for all privileged accounts | Azure AD or AWS IAM with role-based policies Audit Logging | Immutable logs for all PHI access and modification | Azure Monitor / AWS CloudTrail with tamper controls API Security | Authenticated, rate-limited, validated endpoints | OAuth 2.0, input schema validation, WAF rules Data Retention | Defined retention schedule with secure deletion | Policy-driven lifecycle management BAA Coverage | All data processors under Business Associate Agreement | Executed agreements with cloud, ASR, and NLP vendors
Apply these controls equally to production, staging, and development environments. PHI used in model testing is still PHI.
Step 7: Integrate with EHR Systems Using FHIR Standards
EHR integration is usually the most underestimated cost and complexity driver in AI voice agent deployments in healthcare. The NLP output is only really useful when it can land in the right patient record, in the correct format.
Use FHIR R4 as the main integration standard if the EHR supports it. If you are dealing with older or legacy systems, build HL7 v2 message transformation layers instead. The key things to cover are: Patient identity matching against a master patient index, not just a name based lookup, encounter level linking so documentation attaches to the correct visit, structured field mapping from the NLP output into EHR template fields, split by department and visit type, idempotent write operations with transaction ID tracking so retries do NOT create duplicate notes, bidirectional error logging with alerting when writes fail.
Epic and Cerner can support FHIR integrations, but the maturity is not the same everywhere. Meditech and Athenahealth often need custom HL7 transformation for most structured documentation writes. Durapid has delivered healthcare software integrations across all four platforms.
Step 8: Put Physician Review in Place with Human-in-the-Loop Controls
No AI scribe output should turn into a legal medical record without physician validation, not ever. This matters for HIPAA, especially under the minimum necessary standard. It also stays a clinical safety requirement.
The review screen should show the AI draft with section-level confidence indicators, sort of like where the system is pretty sure and where it is not. Low confidence entities should get visual flags so the physician can prioritize the places that need attention fast. Every edit, change, or deletion made during review should be tracked before anything gets finalized.
The edited data, once you strip out identifiers, should feed back into the model improvement pipeline. That way the system learns from real clinician corrections, not just raw text.
Organizations that use structured review workflows typically report physician adoption rates around 78–84%. That’s versus 41–52% when physicians have to work through systems that feel unfamiliar or harder to review (KLAS Research, 2024).
Key Benefits: What Organizations Using AI Clinical Documentation Actually Measure
The claims around medical AI can be a bit vague, sure. Here is what the documented deployments show, in practice, not just in slides or headlines:
Physicians using ambient AI scribe tools often cut documentation time by 35–50 minutes per day on average (AMA, 2024). EHR note completeness scores tend to improve by 31% within the first 90 days of deployment. After-hours pajama time, the industry term for charting done at home after clinic hours, drops by 64% in health systems with deployed medical virtual assistants. Patient interaction time during visits goes up by about 7 minutes per consultation on average when physicians aren’t also typing at the same time. Burnout scores on standardized measures fall by 19% within six months after ambient documentation deployment (Stanford Medicine, 2024).
Still, nobody guarantees any of these results. Virtual medical assistants only hit these numbers when model performance is solid and EHR integration is clean. Clinical adoption has to actually happen too, not only the tech being in place.
Common Failure Modes: What Goes Wrong in Medical Voice AI Deployments
Most competitor blogs describe what works. But figuring out failure modes is pretty much as important, for teams making build or buy decisions, even if it sounds less exciting.
Model Confidence Without Model Accuracy
There is this thing about model confidence without model accuracy. AI scribes can spit out confident, neatly formatted notes that still carry clinical errors. Like a medication dosage transcribed incorrectly, or a negation missed in context, and suddenly you are looking at a patient safety issue, not just a “quality” problem. Specialty-specific benchmark testing should happen before any clinical use, not only some generic WER scoring.
Integration as an Afterthought
Teams that set up the transcription and NLP layers first, then start EHR integration later, often realize their data structures do not map cleanly to the target EHR schema. Design data models with the EHR output format in mind from the very beginning, not as a late add-on.
Security Drift After Launch
Teams test compliance controls at launch and then kind of forget about them. Access policies pick up exceptions over time, logs pile up without review, and nobody notices until it is too late. Quarterly security reviews should be scheduled, with automated compliance monitoring folded into the operations runbook, so it is not a one time checkbox.
Specialty Mismatch
If a model gets fine-tuned on primary care consultations and then gets deployed in oncology, results can get rough fast. The vocabulary, documentation structure, and even conversation patterns are just fundamentally different. Specialty coverage should be scoped carefully, with each specialty validated independently. Otherwise you end up defending a system that was never really trained for that context.
Build Your HIPAA-Compliant Medical Voice Assistant with Durapid
Durapid Technologies builds HIPAA-compliant medical voice assistants and AI clinical documentation systems for healthcare organizations requiring secure, scalable, and enterprise-ready healthcare software solutions. Their team supports everything from Azure OpenAI integrations and EHR connectivity to compliance architecture, NLP fine-tuning, and post-deployment AI governance for real-world clinical environments.
FAQs
How long does it take to build a HIPAA-compliant medical voice assistant from scratch?
Most HIPAA-compliant medical voice assistant platforms take around 5 to 9 months to move from planning to deployment. The timeline depends heavily on compliance setup, EHR integrations, and clinical validation requirements.
What medical speech recognition software is used in production healthcare AI systems?
Most healthcare AI systems use Azure Speech Services, AWS Transcribe Medical, or fine-tuned Whisper models combined with custom medical vocabulary training. Medical voice recognition software of this kind also typically layers custom pronunciation lexicons on top. Generic speech engines alone are usually not accurate enough for clinical environments.
What is the difference between an AI scribe and an AI medical scribe?
An AI scribe simply transcribes conversations. An AI medical scribe, on the other hand, understands clinical terminology, structures documentation like SOAP notes, and integrates securely with EHR systems under HIPAA compliance standards.
What are the HIPAA requirements that specifically apply to voice AI in healthcare?
Healthcare voice AI systems must encrypt patient data, maintain audit logs, and implement role-based access controls. They also need to sign BAAs with vendors and securely manage audio and transcript retention to stay HIPAA compliant.
Can virtual medical assistants handle multiple specialties on a single model?
Yes, but most production systems use specialty-specific fine-tuning layers. Clinical language and workflows vary significantly across departments like cardiology, dermatology, and psychiatry.
Recent Blog